OPINION
Federal, state Medicaid cuts are the real ‘death panels’
By BRENDAN WILLIAMS
(May 10, 2017) — When the Affordable Care Act was debated in Congress, many falsely characterized as “death panels” the once-bipartisan idea of voluntary consultations about hospice and other end-of-life care options. Sarah Palin popularized the term, writing that “the sick, the elderly and the disabled” — including her own child with Down Syndrome — would have to prove they were “worthy of health care.”
The language giving rise to the accusation was removed, but Palin’s observation about those who would “ration care” could today be accurately applied to Congress and state legislatures that are seeking to cut Medicaid for the most vulnerable. The American Health Care Act, which narrowly passed the House last week, is an outright assault upon traditional Medicaid, which covers more than 60% of nursing home residents.

During floor debate on the original version of the AHCA, Rep. Sander Levin (D-Mich.) raised the specter of “elderly evicted from nursing homes, losing coverage from Medicaid, the largest source of long-term care in our nation.” The bill would cut Medicaid more than $800 billion by replacing open-ended funding with per-capita caps that would limit enrollment, and would fall heavily upon those with disabilities.
The revised GOP plan rushed through last week includes the same deep cuts as the original AHCA. And as The Texas Tribune recently noted, “Emboldened by the election of President Donald Trump, Texas House budget writers voted to cut $1 billion in state funding for Medicaid” — with lost federal matching funds, the total cut to care would be $2.4 billion.
 Medicaid, which serves poor and low-income Americans, suffers neglect in good times as well as bad. In New Hampshire, the state has proposed freezing the long-term care appropriation for two years, despite a gap between Medicaid payments and nursing care costs that is already the nation’s third worst at over $50 per patient, per day. Underfunded providers are beset trying to both recruit and retain caregivers in the state with the lowest unemployment rate. Yet while unwilling to assist nursing home care, the state gave prison caregivers a 15% wage increase.
Medicaid, which serves poor and low-income Americans, suffers neglect in good times as well as bad. In New Hampshire, the state has proposed freezing the long-term care appropriation for two years, despite a gap between Medicaid payments and nursing care costs that is already the nation’s third worst at over $50 per patient, per day. Underfunded providers are beset trying to both recruit and retain caregivers in the state with the lowest unemployment rate. Yet while unwilling to assist nursing home care, the state gave prison caregivers a 15% wage increase.
In an aging society, these trends are unsustainable. In its annual report to Congress, the Medicare Payment Advisory Commission (MedPAC) noted that the average nursing home was only running a positive margin, or profit, of 1.6% in 2015. And with Medicare payments excluded, margins were actually negative at -2%. Medicare, the federal program for seniors, only covers nursing home care following a qualifying hospital stay. But its payments are more generous than Medicaid, and for many facilities they make the difference between solvency and closure.
MedPAC complains about this cross-subsidization, writing, “Medicare’s high payments represent a subsidy of trust fund dollars (and taxpayer support) to the low payments made by states and private payers.” It fears a vicious cycle where Medicare rate increases simply mean “states could be encouraged to reduce their Medicaid payments and, in turn, create pressure to raise Medicare rates.”
Yet the buck has to stop somewhere, and neither the federal government nor states appear ready to own the costs of longevity. Providers are caught in the middle. Forced to adhere to very high regulatory standards, they are, year after year, entirely subject to the vagaries of politics. It is no wonder that, amidst perennial uncertainty, so many independent family-owned facilities have been sold to chains or real estate investment trusts.
The latest responsibility-shedding trend may worsen matters, as more states turn over the keys to Medicaid programs to managed care insurers. It is impossible to understand how nursing home care, already operating at a negative margin for Medicaid, can survive a further diversion of Medicaid resources to managed care profits. And the price of failure can be catastrophic. As a private consultant, the new administrator of the Centers for Medicare and Medicaid Services, Seema Verma, designed an Iowa managed care system with disastrous new administrative burdens, payment delays and denials for providers — along with massive state cost overruns. In response to Verma’s work, the Des Moines Register published an editorial headlined, “Providers’ Medicaid nightmare becomes reality.”
Where is the outrage about health care “rationing” and “death panels” when we need it?
 Brendan Williams is the president and CEO of the New Hampshire Health Care Association, which represents 90 long-term care facilities. Roughly 55% of residents at its member nursing homes are on Medicaid. Williams is a former State Representative from Washington’s 22nd Legislative District. This column originally appeared in the USA Today and is cross-posted here with the author’s permission.
Brendan Williams is the president and CEO of the New Hampshire Health Care Association, which represents 90 long-term care facilities. Roughly 55% of residents at its member nursing homes are on Medicaid. Williams is a former State Representative from Washington’s 22nd Legislative District. This column originally appeared in the USA Today and is cross-posted here with the author’s permission.



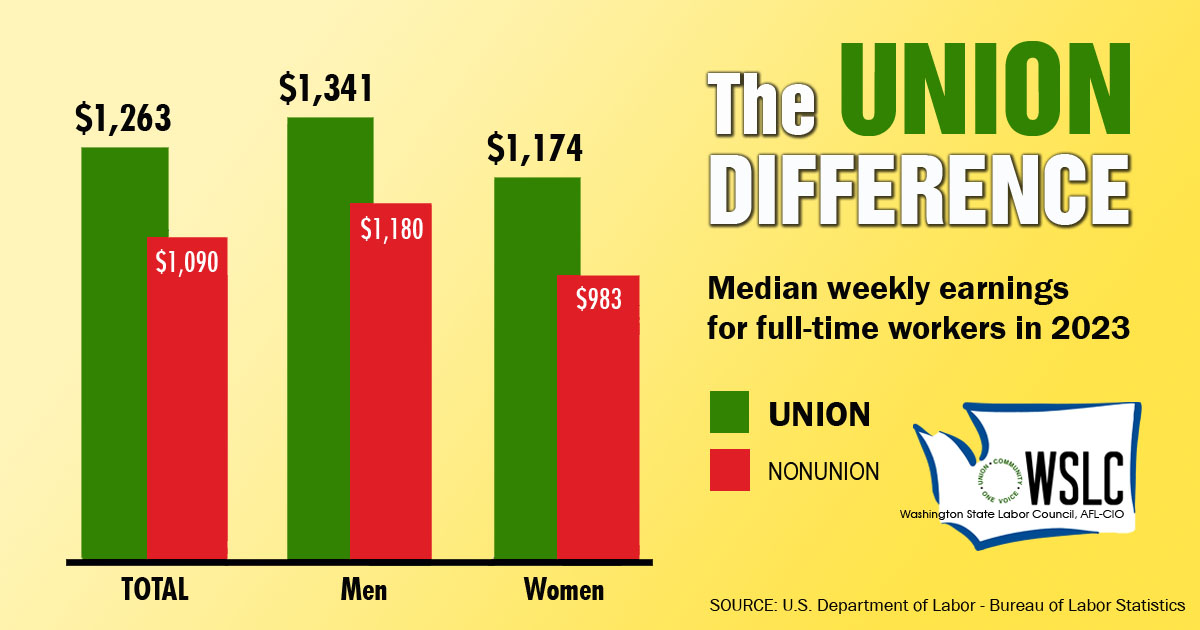
CHECK OUT THE UNION DIFFERENCE in Washington: higher wages, affordable health and dental care, job and retirement security.
FIND OUT HOW TO JOIN TOGETHER with your co-workers to negotiate for better wages, benefits, and a voice at work. Or go ahead and contact a union organizer today!
